


 Sign Out
Sign Out

Glucophage XR: Pharmacotherapeutic Group: ORAL ANTI-DIABETICS. ATC code: A10BA02: Gastrointestinal tract and metabolism.
Pharmacology: Pharmacodynamics: Mechanism of action: Metformin is a biguanide with antihyperglycaemic effects, lowering both basal and postprandial plasma glucose. It does not stimulate insulin secretion and therefore does not produce hypoglycaemia. Metformin may act via 3 mechanisms: reduction of hepatic glucose production by inhibiting gluconeogenesis and glycogenolysis; in muscle, by increasing insulin sensitivity, improving peripheral glucose uptake and utilisation; and delay of intestinal glucose absorption.
Metformin stimulates intracellular glycogen synthesis by acting on glycogen synthase. Metformin increases the transport capacity of all types of membrane glucose transporters (GLUT) known to date.
Pharmacodynamic effects: In clinical studies, use of metformin was associated with either a stable body weight or modest weight loss.
In humans, independently of its action on glycaemia, immediate release metformin has favourable effects on lipid metabolism. This has been shown at therapeutic doses in controlled, medium-term or long-term clinical studies: immediate release metformin reduces total cholesterol, LDL cholesterol and triglyceride levels.
A similar action has not been demonstrated with the extended release formulation, possibly due to the evening administration, and an increase in triglycerides may occur.
Clinical efficacy: Treatment of type 2 diabetes mellitus: The prospective randomised (UKPDS) study has established the long-term benefit of intensive blood glucose control in overweight type 2 diabetic patients treated with immediate release metformin as first-line therapy after diet failure. Analysis of the results for overweight patients treated with metformin after failure of diet alone showed: a significant reduction of the absolute risk of any diabetes-related complication in the metformin group (29.8 events/1000 patient-years) versus diet alone (43.3 events/1000 patient-years), p=0.0023, and versus the combined sulphonylurea and insulin monotherapy groups (40.1 events/1000 patient-years), p=0.0034; a significant reduction of the absolute risk of diabetes-related mortality: metformin 7.5 events/1000 patient-years, diet alone 12.7 events/1000 patient-years, p=0.017; a significant reduction of the absolute risk of overall mortality: metformin 13.5 events/1000 patient-years versus diet alone 20.6 events/1000 patient-years (p=0.011), and versus the combined sulphonylurea and insulin monotherapy groups 18.9 events/1000 patient-years (p=0.021); a significant reduction in the absolute risk of myocardial infarction: metformin 11 events/1000 patient-years, diet alone 18 events/1000 patient-years (p=0.01).
For metformin used as second-line therapy, in combination with a sulphonylurea, benefit regarding clinical outcome has not been shown.
In type 1 diabetes, the combination of metformin and insulin has been used in selected patients, but the clinical benefit of this combination has not been formally established.
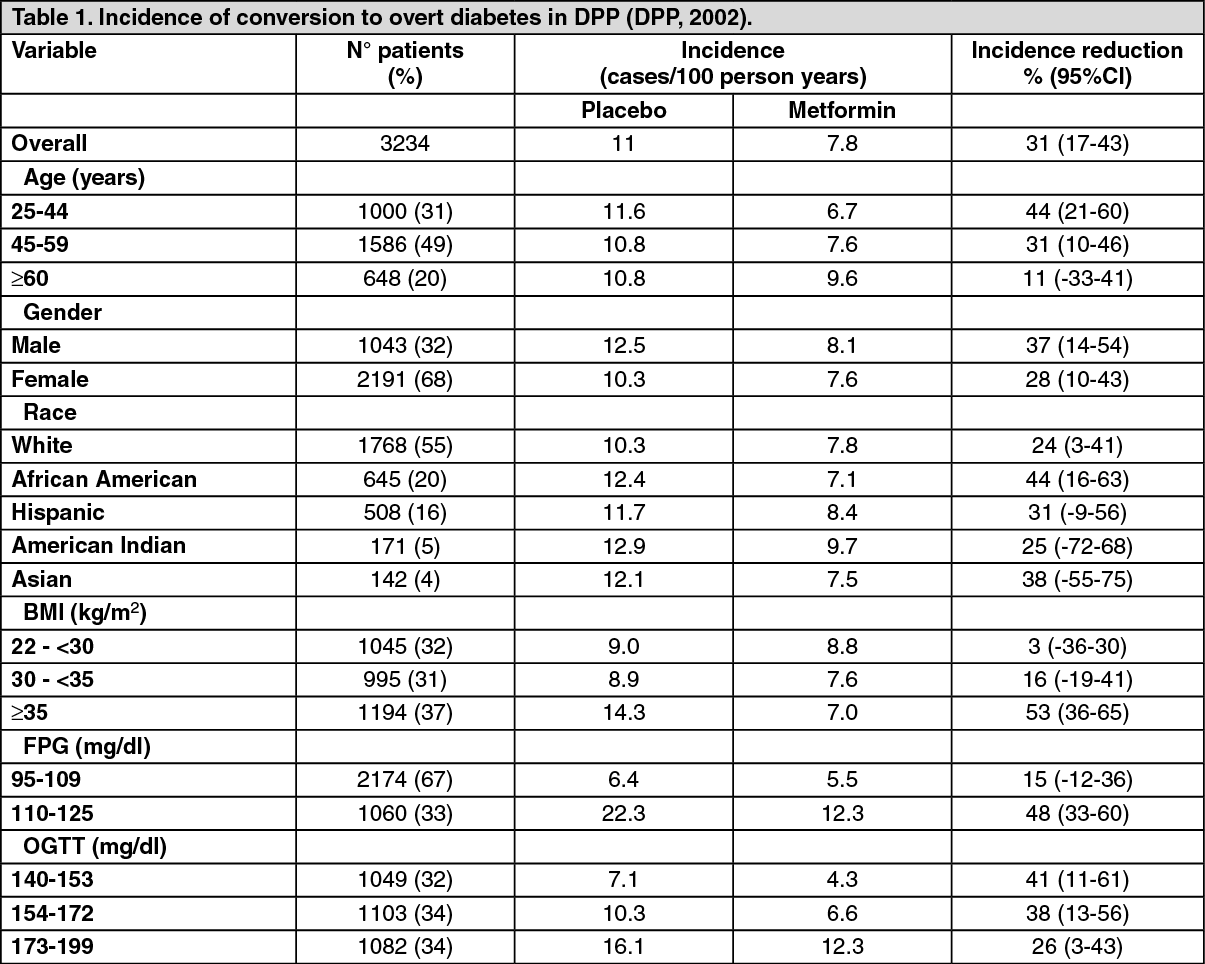
Glucophage XR: Reduction in the risk or delay of type 2 diabetes mellitus: The Diabetes Prevention Program (DPP) was a multicenter randomised controlled clinical trial in adults assessing the efficacy of an intensive lifestyle intervention or metformin to prevent or delay the development of type 2 diabetes mellitus. Inclusion criteria were age ≥25 years, BMI ≥24 kg/m2 (≥22 kg/m2 for Asian-Americans), and impaired glucose tolerance plus a fasting plasma glucose of 95 - 125 mg/dl (or ≤125 mg/dl for American Indians). Patients were either treated with intensive lifestyle intervention, 2x850 mg metformin plus standard lifestyle change, or placebo plus standard lifestyle change.
The mean baseline values of the DPP participants (n=3,234 for 2.8 years) were age 50.6±10.7 years, 106.5±8.3 mg/dl fasted plasma glucose, 164.6±17.0 mg/dl plasma glucose two hours after an oral glucose load, and 34.0±6.7 kg/m2 BMI.
Intensive lifestyle intervention as well as metformin significantly reduced the risk of developing overt diabetes compared to placebo, 58% (95% CI 48-66%) and 31% (95% CI 17-43%), respectively.
The advantage of the lifestyle intervention over metformin was greater in older persons.
The patients who benefited most from the metformin treatment were aged below 45 years, with a BMI equal or above 35kg/m2, a baseline glucose 2 h value of 9.6-11.0 mmol/l, a baseline HbA1c equal or above 6.0% or with a history of gestational diabetes. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTo prevent one case of overt diabetes during the three years in the whole population of the DPP, 6.9 patients had to participate in the intensive lifestyle group and 13.9 in the metformin group. The point of reaching a cumulative incidence of diabetes equal to 50% was delayed by about three years in the metformin group compared to placebo.
The Diabetes Prevention Program Outcomes Study (DPPOS) is the long-term follow-up study of the DPP including more than 87% of the original DPP population for long-term follow up.
Among the DPPOS participants (n=2776), the cumulative incidence of diabetes at year 15 is 62% in the placebo group, 56% in the metformin group, and 55% in the intensive lifestyle intervention group. Crude rates of diabetes are 7.0, 5.7 and 5.2 cases per 100 person-years among the placebo, metformin, and intensive lifestyle participants, respectively. Reductions in the diabetes risk were of 18% (hazard ratio (HR) 0.82, 95% CI 0.72-0.93; p=0.001) for the metformin group and 27% (HR 0.73, 95% CI 0.65-0.83; p<0.0001) for the intensive lifestyle intervention group, when compared with the placebo group. For an aggregate microvascular endpoint of nephropathy, retinopathy and neuropathy, the outcome was not significantly different between the treatment groups, but among the participants who had not developed diabetes during DPP/DPPOS, the prevalence of the aggregate microvascular outcome was 28% lower compared with those who had developed diabetes (Risk Ratio 0.72, 95% CI 0.63-0.83; p<0.0001). No prospective comparative data for metformin on macrovascular outcomes in patients with IGT and/or IFG are available.
Published risk factors for type 2 diabetes include: Asian or black ethnic background, age above 40, dyslipidaemia, hypertension, obesity or being overweight, age, 1st degree family history of diabetes, history of gestational diabetes mellitus, and polycystic ovary syndrome (PCOS).
Consideration must be given to current national guidance on the definition of prediabetes.
Patients at high risk should be identified by a validated risk-assessment tool.
Paediatric population: Glucophage: Controlled clinical studies in a limited paediatric population aged 10-16 years treated during 1 year demonstrated a similar response in glycaemic control to that seen in adults.
Pharmacokinetics: Absorption: Glucophage: After an oral dose of metformin, maximum plasma concentration (Cmax) is reached in approximately 2.5 hours (Tmax). Absolute bioavailability of a 500 mg or 850 mg metformin tablet is approximately 50-60 % in healthy subjects. After an oral dose, the non-absorbed fraction recovered in faeces was 20-30 %.
After oral administration, metformin absorption is saturable and incomplete. It is assumed that the pharmacokinetics of metformin absorption is non-linear.
At the usual metformin doses and dosing schedules, steady state plasma concentrations are reached within 24 to 48 hours and are generally less than 1 microgram/mL. In controlled clinical trials, maximum metformin plasma levels (Cmax) did not exceed 5 microgram/mL, even at maximum doses.
Food decreases the extent and slightly delays the absorption of metformin tablets. Following administration of a dose of 850 mg, a 40 % lower plasma peak concentration, a 25 % decrease in AUC (area under the curve) and a 35 minute prolongation of time to peak plasma concentration were observed. The clinical relevance of these decreases is unknown.
Glucophage XR: After an oral dose of Glucophage XR 500 mg, metformin absorption is significantly delayed compared to the immediate-release tablet (Tmax at 2.5 hours) with a Tmax at 7 hours.
Following a single oral administration of 1500 mg of Glucophage XR 750 mg, a mean peak plasma concentration of 1193 ng/mL is achieved with a median value of 5 hours and a range of 4 to 12 hours. Glucophage XR 750 mg was shown to be bioequivalent to Glucophage XR 500 mg at a 1500 mg dose with respect to Cmax and AUC in healthy fed and fasted subjects.
Following a single oral administration in the fed state of one tablet of Glucophage XR 1000 mg, a mean peak plasma concentration of 1214 ng/mL is achieved with a median time of 5 hours (range of 4 to 10 hours). Glucophage XR 1000 mg was shown to be bioequivalent to Glucophage XR 500 mg at a 1000 mg dose with respect to Cmax and AUC in healthy fed and fasted subjects.
At steady state, similar to the immediate-release formulation, Cmax and AUC are not proportionally increased to the administered dose. The AUC after a single oral administration of 2000 mg metformin prolonged-release is similar to that observed after administration of 1000 mg metformin immediate-release twice daily.
Intrasubject variability of Cmax and AUC of metformin prolonged-release is comparable to that observed with metformin immediate-release.
When 2 tablets of 500 mg metformin prolonged-release is administered in fed conditions the AUC is increased by approximately 70% (both Cmax and Tmax are only slightly increased).
When the 1000 mg prolonged release tablet are administered in fed conditions the AUC is increased by 77% (Cmax is increased by 26% and Tmax is slightly prolonged by about 1 hour).
Metformin absorption from the prolonged-release formulation is not altered by meal composition.
No accumulation is observed after repeated administration of up to 2000 mg metformin prolonged-release.
Distribution: Plasma protein binding is negligible. Metformin partitions into erythrocytes. The blood peak is lower than the plasma peak and appears at approximately the same time. The red blood cells most likely represent a secondary compartment of distribution. The mean volume of distribution (Vd) ranged between 63-276 L.
Metabolism: Metformin is excreted unchanged in the urine. No metabolites have been identified in humans.
Elimination: Renal clearance of metformin is > 400 ml/min, indicating that metformin is eliminated by glomerular filtration and tubular secretion. Following an oral dose, the apparent terminal elimination half-life is approximately 6.5 hours.
When renal function is impaired, renal clearance is decreased in proportion to that of creatinine and thus the elimination half-life is prolonged, leading to increased levels of metformin in plasma.
Paediatric Population: Glucophage: Single dose study: After single doses of metformin 500 mg, paediatric patients have shown similar pharmacokinetic profile to that observed in healthy adults.
Multiple dose study: Data are restricted to one study. After repeated doses of 500 mg twice daily for 7 days in paediatric patients the peak plasma concentration (Cmax) and systemic exposure (AUC0-t) were reduced by approximately 33% and 40%, respectively compared to diabetic adults who received repeated doses of 500 mg BID for 14 days. As the dose is individually titrated based on glycaemic control, this is of limited clinical relevance.
Toxicology: Preclinical safety data: Preclinical data reveal no special hazard for humans based on conventional studies on safety, pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity reproduction.